Who Uses RBRVS EZ-Fees?

Providers
- Physicians and other healthcare professionals

Payers
- Insurance companies
- Federal health plans
- State Agencies
- Managed care
- (HMO, PPO, TPA, PHO, IPA)

Administrators
- Office managers
- Consultants
- Accountants
- Billing services
- 3rd Party Administrators
- CFOs, CEOs, and CPAs

Other Interested Parties
- Life care planners
- Actuaries
- Lawyers
- Medical societies
- State and Federal agencies
Introductory Video
RBRVS, or resource-based relative value scale, is a structured and scalable payment system used by CMS (Medicare/Medicaid), many state workers compensation boards, and nearly all HMO’s (health maintenance organizations). It is a fairly complicated system to navigate without help. RBRVS EZ-Fees is a low cost PC software application that simplifies RBRVS with one main screen and no complicated manuals or training. With a few clicks you can look up any medical fee for over 10,000 payment localities.
Note, Medicare does not pay for all CPT/HCPCS services by not assigning (RVUs) relative value units. Codes not valued by Medicare are referred to as gap codes. As an added value, RBRVS EZ-Fees offers an optional gap license.
Since 1998, RBRVS EZ-Fees has helped thousands of healthcare professionals simplify the Medicare payment formula.
With a few clicks you can create medical fee schedules without government downloads or complicated formulas. Most users have mastered our software in 5 minutes!

What are people saying about us?
 Bob Shuman
Bob Shuman
Hebrew Rehabilitation Center for Aged
“I just wanted to re-emphasize the value of the above-referenced product. Again, its ease of use, flexible views and condensed information really makes this product a valuable tool.”
David V
“I have been using EZ-Deposit since 2007. It has been a great way to track deposits and has saved me from having to purchase deposit slips! Great product!”
Judith Southworth
Virginia Health Network
“I have used your EZ-Fees product now for 5 years. I am not a technical person and the product is so simple to use and it does exactly what I need to create multiple fee schedules quickly and easily. The addition of the gap codes is a real plus! We used a different product for several years before we found your product and have had other companies send us marketing materials for their products. None have caused us to try anything else. Thank you again for your product and your support through these many years.”
Douglas C. Anderson
MarketGuild
“EZ Fees is simple, elegant, and versatile and is comparable to products costing many thousands of dollars more! It is a “must” for anyone who works with Medicare fees or is engaged in fee schedule building or analysis. In one package all of the principal office based Medicare payment systems are at you fingertips. The data alone in EZ Fees is worth the acquisition cost. Simply the best product of its kind in the market!””
Ken Nelson
MONEYRULE$
“RBRVS EZ-Fees is superb for creating dynamic variables by specialties or payer schedules linked to frequencies. Just change the Fee Manager percentage and click. Viewing several fees at the same time helps valuation of contracts too.”
Jaqueline Nossig, Billing Manager
Pain Manager Center of Wisconsin
“RBRVS EZ-Fees has been excellent for creating and verifying all our RBRVS based fee schedules and contracts. We just select a percent increase in Fee Manager and click a button. No more formulas and government downloads. Since using EZ-Fees we found codes that we should have been using and increased our revenue by 5-7%. In a medical practice that means thousand of dollars annually.”
John P House, RN, MBA
Practice Administrator
The Lincoln Pediatric Group, LLC
“I just wanted to take a minute to tell you how much I love your product. I use it to prepare fee schedules so that I can double check to see that the insurance companies are paying me properly. I had looked at other products, but they either didn’t do what I wanted, or they did lots more than I needed, and were therefore, much more expensive than RBRVS EZ-Fees. I wish I would have known about this product years ago. It is perfect for the physician office administrator looking to make fee schedule preparation easier for a reasonable cost. Thanks for a great product at an affordable price.”
Cherice Cottrell, Director of Operations
Leslie R. Coffman, MD
“Your software is delightfully easy to use: transparent, concise, and straightforward. EZ-Fees has made converting and verifying my Medicare-based fees schedules a breeze! Thanks for a great product.”
If you’re not using the latest RVUs and CF you may be leaving money on the table.
No messy government downloads or complicated formulas. Let us keep you up-to-date with the #1 RBRVS solution on the market.

Take A Quick Tour
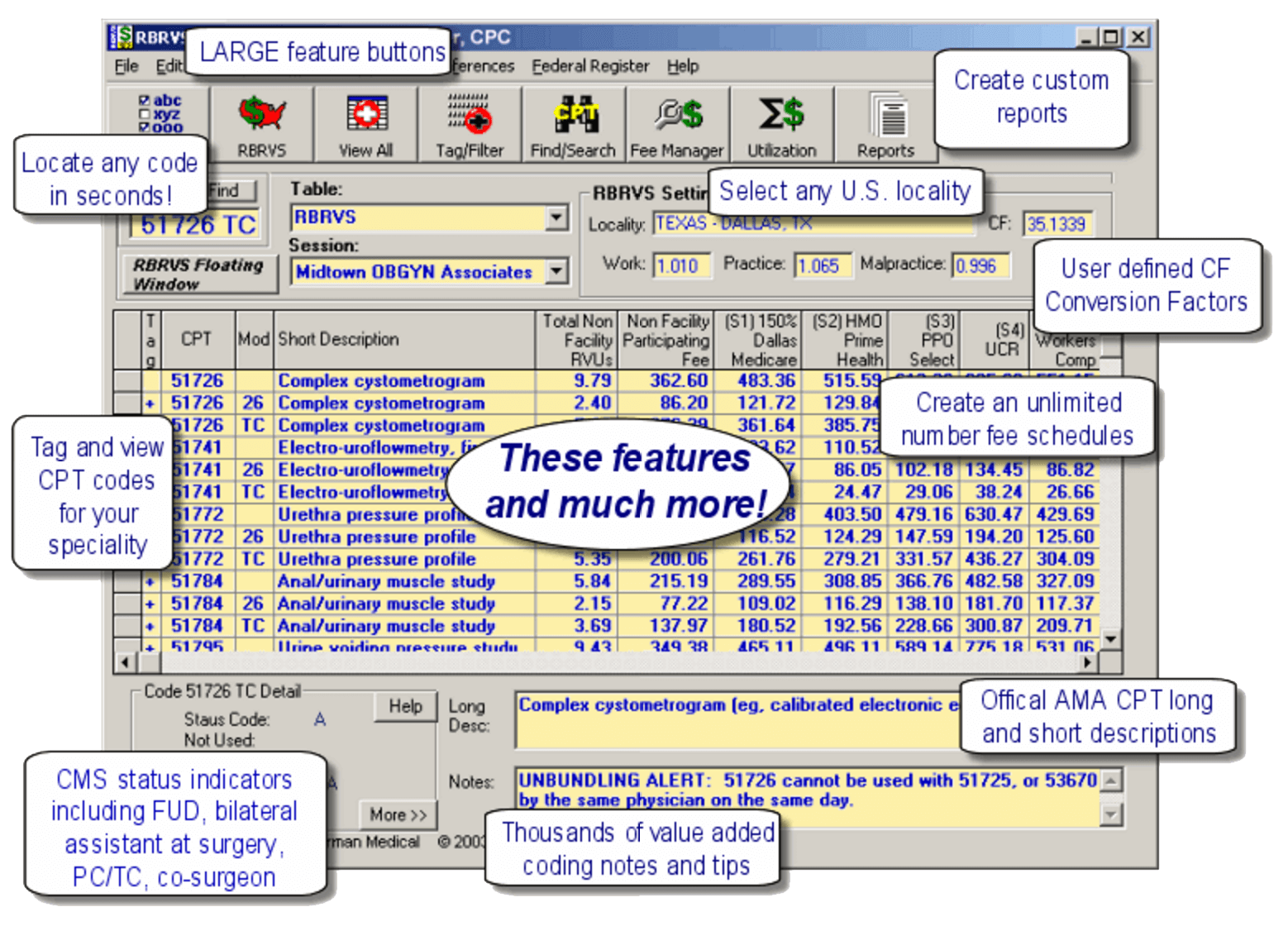
The red button of the U.S. allows the user to look up and select a Medicare locality. The Select by State tab allows lookups by state, city, county, Part B carrier, locality, and browse work, practice and malpractice GPCIs.
See second image for Select by Zip Code Tab
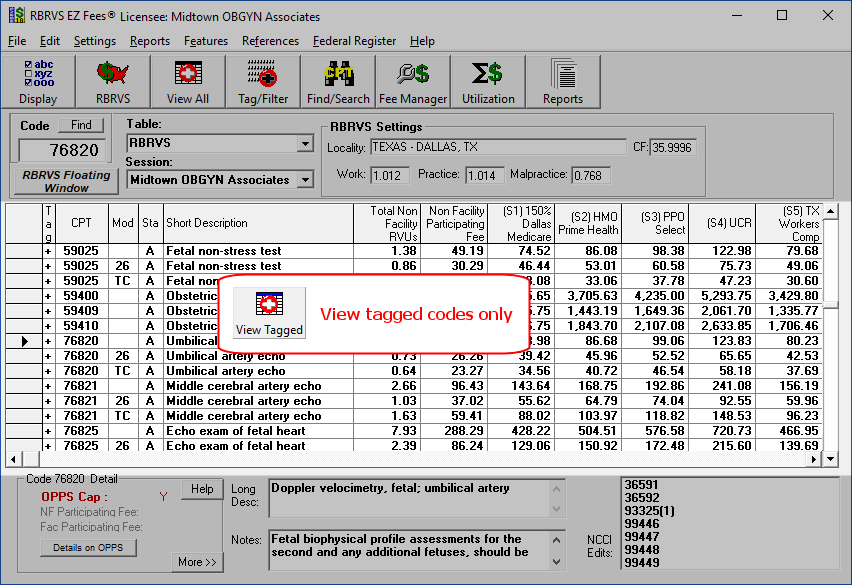
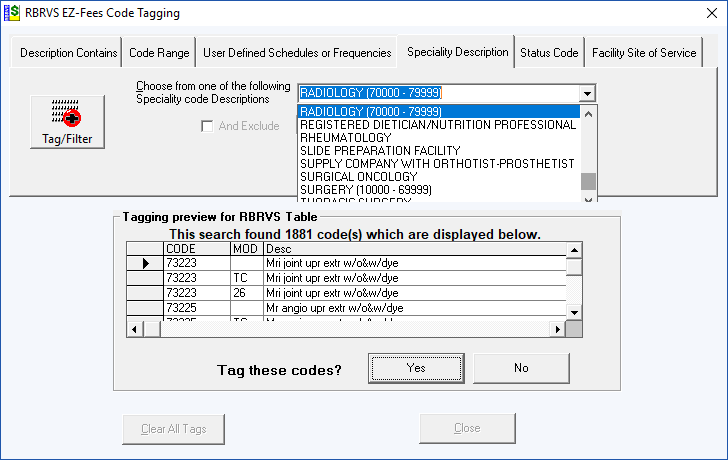
The View Tagged button allows for viewing tagged codes only. Tagging allows you to select only those code you are interested in viewing or printing. Tagged codes have a “+” sign on the main screen.
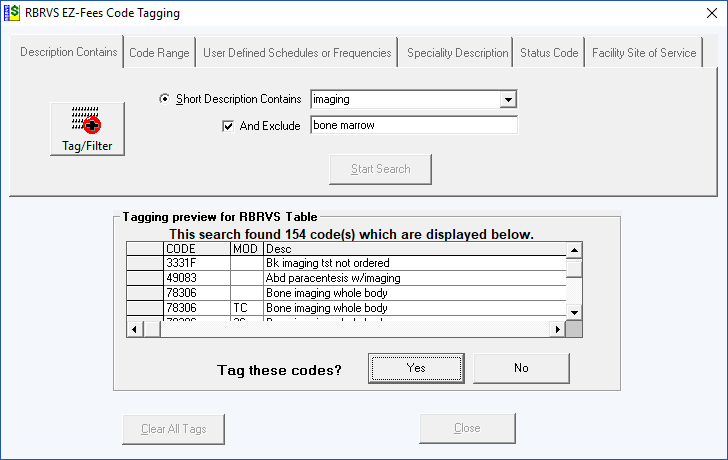
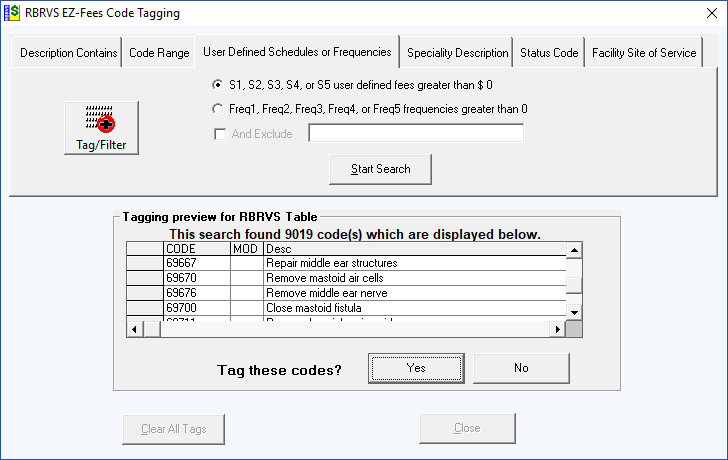
The Tag/Filter button allows for tagging (book marking) procedure codes based on Description, Code Range, Fee or Frequency Values, Medical Specialty and Code Status. Tagged codes can then be selected to be viewed only on the main screen and printed. Tagging is cumulative – meaning you can make several passes to tag additional codes that meet different search criteria. You can clear, save and load a tag list. RBRVS EZFees contains several tagging methods.
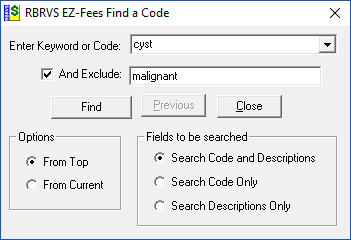
The Find / Search button searches for any keyword or code with several options to assist in locating difficult to find codes. The dropdown list hold the last 10 keywords.
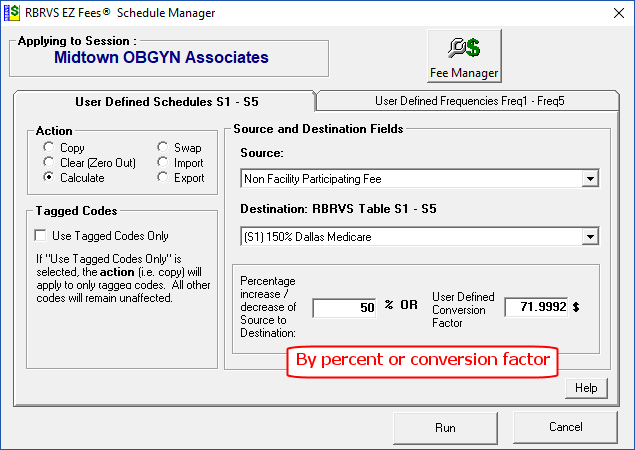
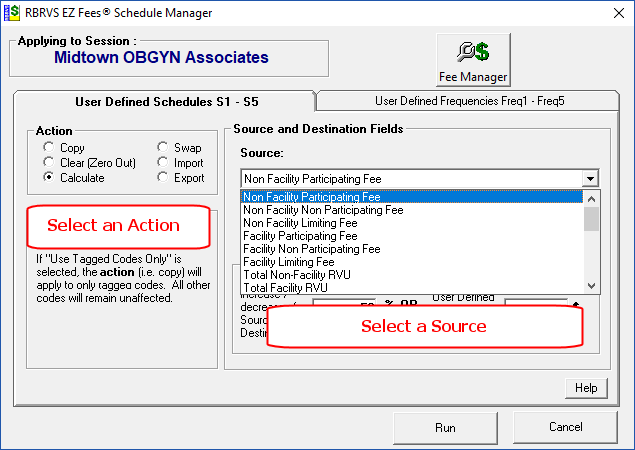
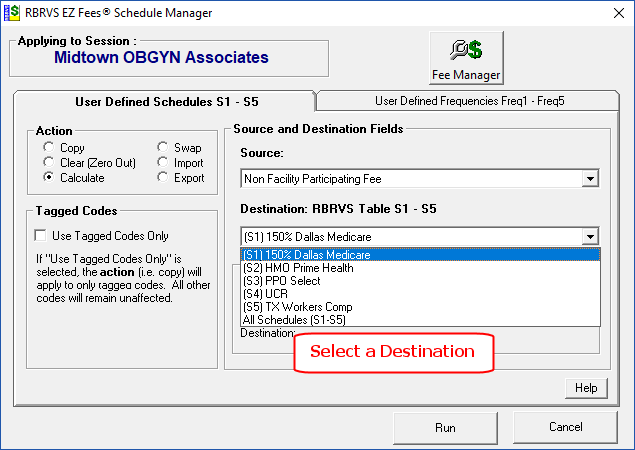
The Fee Manager button allows the user to create and modify fee schedules. In this example, the user is creating a fee schedule called Dallas Medicare that is above the Non participating Medicare Fee Schedule for Dallas, Texas.
The “Source” can be any of the 6 Medicare Fee Schedules or any of the 5 User Defined Fee Schedules.
The “Destination” is any of the 5 User defined Fee Schedules
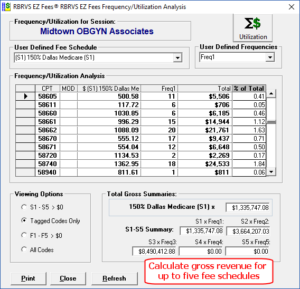
There are two tabs in the Schedule Manager: Fee Schedules and Frequency Schedules. You can perform the same operations on up to 5 User Define Frequency Schedules.
The Utilization / Frequency feature shows procedure code, selected user defined fee and frequency schedule and total (user defined fee time frequency and percent of total schedule).
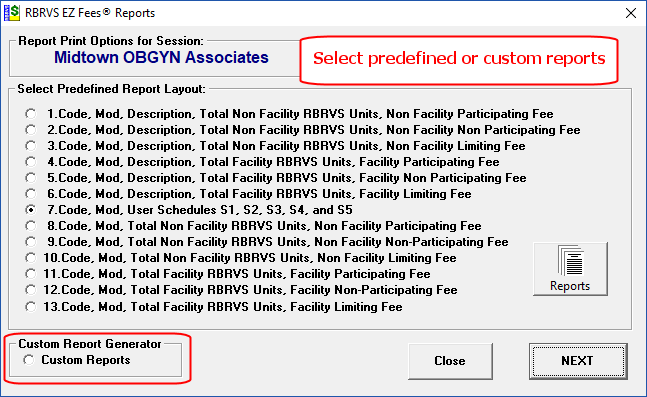
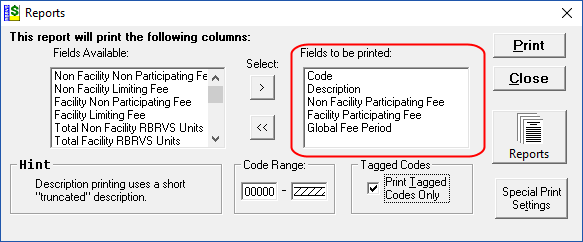
The Reports button brings up 13 common pre-defined report layouts.For custom reports select the “Custom Reports” option. Custom Reports allows for user defined fields. The “Print Tagged Codes Only” check box is an excellent way to print only those codes you wish to include in your report.